
Image courtesy of alimedial.com
What is FEES?
For years, Medical Doctors and Speech-Language Pathologists were only able to diagnostically analyze swallowing disorders via Videofluoroscopy (VFSS), which is also known as a Modified Barium Swallow Study (MBSS). This test is good at highlighting many aspects of a person's swallow, but in the past 20 years, medical technology has evolved greatly, and there have been major breakthroughs in the field of diagnostic imaging.
The Flexible Endoscopic Evaluation of Swallowing (FEES) procedure has risen to become a gold standard in the field of medicine, gastroenterology, speech-language pathology, otorhinology and dysphagia; research has shown FEES to be one of the most sensitive and specific tools for identifying aspiration and penetration. In a 2010 comparison study of MBSS/VFSS and FEES in children (conducted by da Silva, Lubianca-Neto and Santoro), the authors noted, "Regarding the analyzed parameters, laryngeal penetration and aspiration yielded the highest interobserver agreement in terms of FEES, and also showed the highest specificity and positive predictive value when compared to VFSS." As well, the authors noted that VFSS/MBSS did not agree well with FEES ("The diagnostic agreement between FEES and VFSS was low").
As well, a 2015 NIH-funded study comparing clinical bedside evaluations with diagnostic imaging for swallowing disorders (conducted by O’Horo, Rogus-Pulia, Garcia-Arguello, Robbins & Safdar) noted "Our results show that most bedside swallow examinations lack the sensitivity to be used as a screening test for dysphagia across all patient populations examined."
We cannot simply be providing bedside evaluations! Research has shown time and time again that clinical bedside swallowing evaluations routinely miss silent aspiration and often end with overly restrictive dietary recommendations. We are decreasing the quality of life of our patients, possible causing some patients to die prematurely and increasing the costs of the health care industry/facilities. At Florida Voice and Swallowing Diagnostics, we do not argue for or against any certain type of swallowing evaluation; we believe a world exists where the most appropriate diagnostic tool will be chosen based on the unique patient's needs (as well as what the medical team is attempting to look for). Like many aspects of medicine, there are a variety of ways or imaging the human body; endoscopy is simply one of those ways. Though there are potential pitfalls of any diagnostic imaging, we believe, broadly speaking, that endoscopy provides an accurate, sensitive and specific way of examining someone's swallowing mechanisms. As well, the variety of current empirical research conducted around the world tends to validate this.
The limitations of VFSS/MBSS
The limitations of VFSS/MBSS are well-documented over the past 20 years:
- MBSS/VFSS uses radioactivity and radiology, which many people dislike.
- MBSS/VFSS is so radioactive that the x-ray machine is only on for brief moments of the swallow; as such, many post-swallowing events are missed (post-swallow residue clearing, post-swallow aspiration, post-swallow penetration, post-swallow esophageal-laryngeal regurgitation).
- MBSS/VFSS is only on for such a short time, and cannot accurately assess fatigue and compensatory strategies in many patients, which is a vitally important aspect to treatment.
- MBSS/VFSS does not directly image the patient's actual anatomy; it completely misses important diagnostic indicators such as swelling, discoloration, anatomical texture or coloration, etc.
- MBSS/VFSS cannot identify soft-tissue degradation from acid refulx (LPR/GERD).
- MBSS/VFSS cannot be used therapeutically and requires a patient to be transported to the radiology suite, which can be a major burden/stress and also be a large cost to a facility.
- MBSS/VFSS requires a patient to be seated in a very specific way, and patients rarely are seated as such when they are normally eating or drinking. As well, MBSS/VFSS requires and food or liquid to be adulterated and mixed with barium contrast (so that it can show up on the X-ray). As such, MBSS/VFSS does not fully provide a truly accurate and functional representation of a person's actual swallowing ability in their normal, functional situation with their normal food, liquid and medication.
- MBSS/VFSS have multiple costs associated with them that fall on the burden of many facilities. As well, the price of barium has tripled in recent years.
FEES IN ACTION
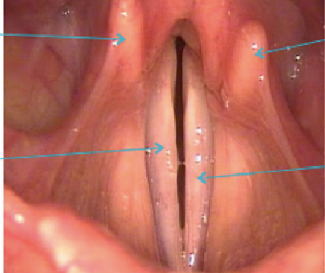
The pictures below are various FEES/Stroboscopy studies via various systems; see the difference yourself!

Larynx during phonatory task.

Note the degradation and edema of the TVFs due to gastric acid.
Larynx during phonatory task.

Larynx and epiglottis during swallowing task.